


Six weeks after quitting, most people feel better. Breathing is easier. The morning cough starts to fade. The lungs have a real capacity to recover. Cilia — the tiny hair-like structures lining the airways that smoking and pollution damage — begin regenerating within weeks of reduced irritant exposure. Airway inflammation subsides. Lung function improves measurably over months.
But recovery doesn’t happen in a vacuum. It happens in whatever air surrounds you. And if that air is still carrying the particles and gases that caused the damage, the recovery process runs into resistance at every step.
What exactly is the lung doing?
Cilia are the lungs’ primary cleaning mechanism — hair-like structures lining the airways that sweep mucus, debris, and particles upward and out. Chronic smoke exposure paralyzes and eventually destroys them. When exposure stops, they begin to regrow.
Between one and three months after quitting, lung function can improve by as much as 30%, with cilia largely restored and mucus clearance working again. The recovery timeline is well-documented and follows a predictable sequence.
The complication is that regenerating cilia are more vulnerable than mature ones. PM2.5 particles landing on new tissue during this window cause the same category of damage that triggered the recovery process in the first place. The body is rebuilding while the exposure continues — at a lower level, perhaps, but continuously.
Inflammation follows a similar pattern. Bronchial inflammation begins declining almost immediately after smoking stops. But that decline depends on what’s in the surrounding air. Fine particles from outdoor pollution entering through windows, from cooking without exhaust ventilation, from a household member smoking elsewhere — any of these sustain the inflammatory state that the lung is working to resolve.
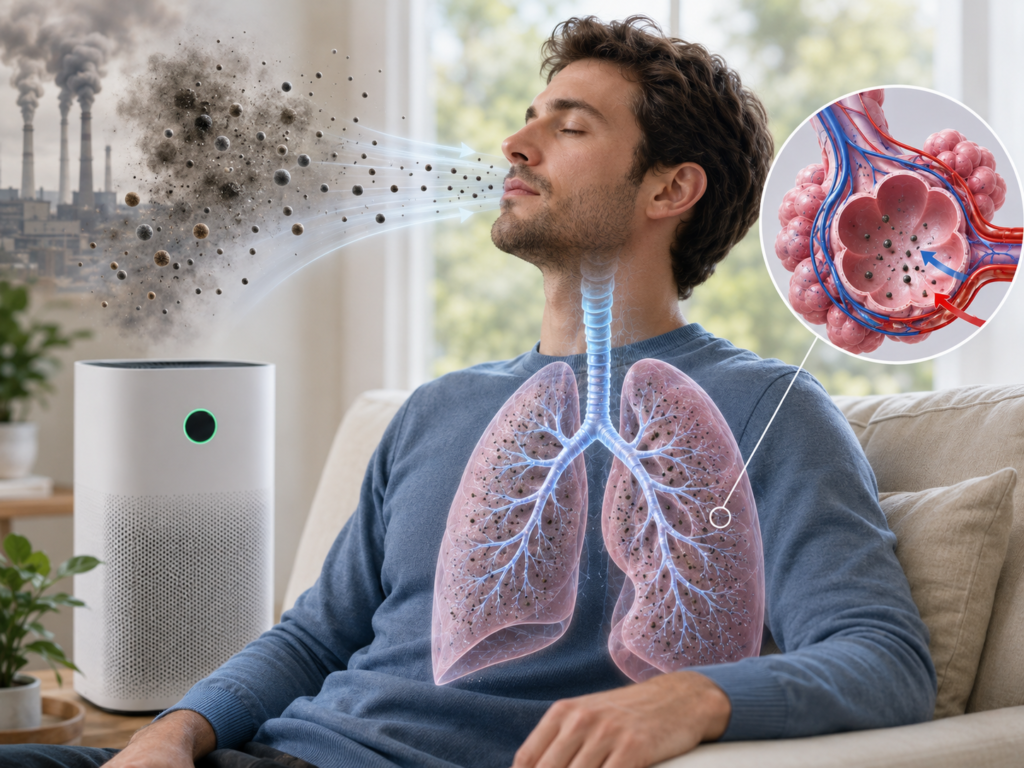
Further down in the lung, macrophages handle particle clearance at the alveolar level. These immune cells physically engulf particles that reach the deep lung. Long-term PM2.5 exposure alters their function at the cellular level, reducing their capacity to do that job. A recovering lung that’s still exposed to high particulate concentrations is depending on immune cells that have already been compromised by the same exposure.
The Clinical Evidence
The relationship between air filtration and respiratory health has been studied in randomized controlled trials — the strongest study design available in clinical research.
The CLEAN AIR Study, conducted at Johns Hopkins and published in the American Journal of Respiratory and Critical Care Medicine, placed two portable HEPA and activated carbon filter units in the homes of former smokers with moderate-to-severe COPD. At six months, participants using active filters reported fewer respiratory symptoms and reduced use of rescue medication. At three months, no measurable difference between groups had emerged.
That three-month lag matters. Filtration doesn’t produce immediate relief. The benefit accumulates over months of sustained reduction in particle exposure — consistent with what’s known about cilia regeneration and inflammation resolution, both of which operate on similar timescales.
A separate study examined children hospitalized for asthma exacerbation. Both groups received standard asthma education; one group also received two HEPA filters for home use. At one year, 30.6% of the filter group reported symptoms in the previous two weeks, compared to 48.6% in the group without filters. Combined unscheduled clinic visits, emergency department visits, and hospitalizations: 11.1% versus 51.4% — a 40-percentage-point gap in healthcare utilization attributable to home air filtration.
The third study was conducted in Beijing, China, on non-smoking older adults., found that two weeks of HEPA purifier use reduced indoor PM2.5 from 60 to 24 µg/m³ and produced measurable reductions in systemic inflammation markers. Environmental intervention, no medication, quantifiable biological effect.
Where the Evidence Has Limits
The clinical data supports air filtration’s role in reducing symptoms and hospitalizations. It does not consistently show improvement in FEV1 — forced expiratory volume, the standard measure of how much air the lungs can move in one second. A separate COPD trial found a 25.2% improvement in heart rate variability among participants using active filters, with no improvement in the placebo group. Heart rate variability is a meaningful health marker, but it isn’t the same as restored lung capacity.
The distinction is important. Filtration appears to reduce inflammatory burden and symptom frequency. It does not appear to reverse structural damage — the permanent airway remodeling from long-term COPD, fibrosis from years of smoke exposure. Those changes reflect physical alterations to lung tissue that cleaner air cannot undo.
For someone in early recovery, or managing reactive airway disease before permanent structural change has occurred, the environment matters more. For someone with advanced emphysema or severe COPD, filtration can reduce discomfort and exposure without restoring capacity that has already been lost.
Why PM2.5 Is the Specific Variable
The benefit observed in these trials runs through PM2.5 reduction. PM2.5 is the most reliable indoor marker of tobacco smoke presence, and indoor PM2.5 levels are directly linked to chronic lung disease progression in the research literature.
Particles at 2.5 microns and below are small enough to bypass upper airway defenses entirely and reach the alveoli — the small sacs where oxygen and carbon dioxide are exchanged. At that depth, fine particles trigger macrophage response, sustained inflammation, and oxidative stress. Reducing their concentration in the breathing environment removes the stimulus keeping those responses active.
H13-grade HEPA removes 99.95% of particles at 0.3 microns, which is the performance level used in the clinical trials described above. MERV-13 filtration — standard in residential HVAC systems — removes 75–85% of particles in that range. For general household air quality, MERV-13 is often sufficient. In a lung recovery context, the difference between 85% and 99.95% particle removal is clinically relevant.
Substances that HEPA filters cannot filter
Clinical attention focuses on HEPA and particulate matter. Gas-phase pollutants are a separate problem that HEPA does not address.
Formaldehyde off-gassing from furniture and flooring. Benzene from cleaning products. Volatile organic compounds from adhesives, paint, and synthetic materials. These compounds pass through HEPA fiber media without being captured — they are gases, not particles, and fiber filtration has no mechanism to stop them.
A healthy respiratory system handles low-level VOC exposure without significant response. An airway in recovery is a different situation. Tissue that’s still inflamed and structurally fragile reacts to chemical irritants that it would otherwise process without difficulty.
Activated carbon addresses the gas phase. Carbon adsorbs VOCs and odors through a surface chemistry mechanism that fiber filtration cannot replicate. In a recovery context, the carbon layer is not a secondary convenience. It is handling a category of pollutant that directly affects recovering tissue.
One practical note: activated carbon has finite adsorption capacity. A saturated carbon layer no longer removes pollutants and, under certain conditions, can begin releasing what it previously captured. In environments with above-average chemical load — recently renovated spaces, homes with a history of indoor smoking, urban apartments with persistent outdoor pollution — carbon filters should be replaced more frequently than the manufacturer’s standard interval, which is calibrated to average household conditions.
The Boundaries
Air filtration has documented benefits for respiratory health. It also has boundaries that are worth stating plainly.
Filtration does not remove carbon dioxide or carbon monoxide. Both require ventilation — physical exchange of indoor and outdoor air. A closed room with an air purifier will accumulate CO₂ regardless of filter quality. Ventilation and filtration address different problems and are not substitutes for each other.
A purifier sized for a smaller space than it’s operating in will not produce meaningful PM2.5 reduction. The clinical studies achieved results by lowering concentrations from 50–60 µg/m³ to below 25 µg/m³ — which requires sufficient clean air delivery rate relative to room volume. A general benchmark: smoke CADR of at least two-thirds the room’s square footage.
Filtration is not medical treatment. COPD, asthma, post-COVID respiratory involvement, and other diagnosed conditions require clinical management. Air quality modification can support the environment in which treatment occurs — it cannot replace the treatment itself. Decisions about environmental interventions for diagnosed respiratory conditions belong in conversation with a physician.










